|
Overview
 It is important to note that pronation is not wrong or bad for you. In fact, our feet need to pronate and supinate to achieve proper gait. Pronation (rolling inwards) absorbs shock and supination (rolling outwards) propels our feet forward. It is our body?s natural shock-absorbing mechanism. The problem is over-pronation i.e. the pronation movement goes too deep and lasts for too long, which hinders the foot from recovering and supinating. With every step, excess pronation impedes your natural walking pattern, causing an imbalance in the body and consequent excessive wear and tear in joints, muscles and ligaments. Some common complaints associated with over-pronation include heel Pain (Plantar Fasciitis), Ball of foot pain, Achilles Tendonitis, Shin splints, Knee Pain, Lower Back Pain. Causes A fallen arch occurs because one of the main structures that support the arch has broken or torn. Usually it occurs without trauma, although a small injury associated with the onset of the pain is often recalled, it is sometimes difficult to determine whether the injury was clearly big enough to permanently injure the leg. I suspect that even before the symptoms that the structure that broke was weakening and the injury was simply the ?needle that broke the camels back?. The structure that is most commonly torn is the posterior tibial tendon. This tendon is attached to a muscle on the inside of the back of the ankle, and runs along the medial malleolus, the bony prominence on the inside of the ankle, to attach to a bone in the arch called the navicular bone. It usually begins to weaken and stretch along the back of the medial malleolus. It often begins as a swelling and the arch flattens over the next several weeks to months. As the arch flattens, other structures that support the arch begin to stretch and tear. The bones along the outside of the ankle begin to crush together, causing pain and swelling in this are, and the toes may tilt to the outside as the arch collapses. It is not known why this process begins. It is often associated with diabetes and rheumatoid arthritis and other inflammatory diseases. It also is more common as a person enters the fifty to seventy year age range. ?Fallen arches? are much more common in people who are already flat footed. Symptoms Most patients who suffer from flat feet or fallen arches often do not complain of any symptoms whatsoever. However, on some occasions, patients may find that their feet are fatigued fairly easily and following activity on long periods of standing may have a painful foot or arch. On occasions, swelling may be seen on the inner aspect of the foot and performing certain movements may be painful and difficult. Some patients who have flat feet may find that their feet tend to roll in (over-pronate) a lot more when they walk and run. As a result, they may experience damage to the ankle joint and the Achilles tendon, as well as excessive shoe wear. Diagnosis You can test yourself to see if you have flat feet or fallen arches by using a simple home experiment. First, dip your feet in water. Then step on a hard flat surface, like a dry floor or a piece of paper on the floor, where your footprints will show. Step away and examine your foot prints. If you see complete/full imprints of your feet on the floor, you may have fallen arches. However, it?s important to seek a second option from a podiatrist if you suspect you have fallen arches so they can properly diagnose and treat you. deelsonheels Non Surgical Treatment Heel cord stretching is an important part of treatment, as a tight Achilles tendon tends to pronate the foot. Orthotics (inserts or insoles, often custom-made) may be used. These usually contain a heel wedge to correct calcaneovalgus deformity, and an arch support. This is the usual treatment for flexible Pes Planus (if treatment is needed). A suitable insole can help to correct the deformity while it is worn. Possibly it may prevent progression of flat feet, or may reduce symptoms. However, the effectiveness of arch support insoles is uncertain. Arch supports used without correcting heel cord contracture can make symptoms worse. In patients with fixed Pes planus or arthropathy, customised insoles may relieve symptoms. Reduce contributing factors, wear shoes with low heels and wide toes. Lose weight if appropriate. Do exercises to strengthen foot muscles - walking barefoot (if appropriate), toe curls (flexing toes) and heel raises (standing on tiptoe). Surgical Treatment  Common indications for surgery are cerebral palsy with an equinovalgus foot, to prevent progression and breakdown of the midfoot. Rigid and painful Pes Planus. To prevent progression, eg with a Charcot joint. Tibialis posterior dysfunction, where non-surgical treatment is unsuccessful. Possible surgical procedures include Achilles tendon lengthening. Calcaneal osteotomy, to re-align the hindfoot. Reconstruction of the tibialis posterior tendon. For severe midfoot collapse of the arch, triple arthrodesis may be indicated. Prevention Donning a first-rate pair of arch supports, therapeutic socks and proper footwear before heading out to enjoy hours of holiday fun is one option to consider. Your podiatrist can help you find just the right ones. Once you have them on, they?ll help ease the amount of pressure being put on your body and keep the blood flowing in the right direction. While you?re standing in line, consider doing a bit of exercise as well. We?re not talking about channeling your inner Jack LaLanne here. Otherwise, you might attract the attention of the mall security guards. Simple ankle rotations and walking in place may help to reduce edema and give your flat feet a bit of a break. If you happen to be in a shopping mall or center where foot massages are available, take advantage of them periodically. They are likely to make you feel better and it?s a great excuse to carve out a few quiet moments for yourself. If you can?t visit a professional, tuck a personal foot massager into your purse. That way, you can lightly massage your own feet during the car ride home. Lastly, there are certain foods and nutritional supplements available that may reduce edema caused by standing on flat feet for hours at a time. The list includes potassium rich foods like raisins, bananas, baby carrots, nuts and yogurt. So, you may want to pack a snack for those trips to the mall or hit the food court before you hit the stores. Overview
Your child has been diagnosed with a leg-length discrepancy. This means that your child?s legs are slightly different lengths, with one leg longer than the other. The difference in lengths can vary widely. The larger the difference in lengths, the more problems that can result as the child gets older. Because of this, your child may be referred to a pediatric orthopedist (doctor specializing in treating bone and joint problems in children) for evaluation and possible treatment.  Causes Common causes include bone infection, bone diseases, previous injuries, or broken bones. Other causes may include birth defects, arthritis where there is a loss of articular surface, or neurological conditions. Symptoms In addition to the distinctive walk of a person with leg length discrepancy, over time, other deformities may be noted, which help compensate for the condition. Toe walking on the short side to decrease the swaying during gait. The foot will supinate (high arch) on the shorter side. The foot will pronate (flattening of the arch) on the longer side. Excessive pronation leads to hypermobility and instability, resulting in metatarsus primus varus and associated unilateral juvenile hallux valgus (bunion) deformity. Diagnosis Asymmetry is a clue that a LLD is present. The center of gravity will shift to the short limb side and patients will try to compensate, displaying indications such as pelvic tilt, lumbar scoliosis, knee flexion, or unilateral foot pronation. Asking simple questions such as, "Do you favor one leg over the other?" or, "Do you find it uncomfortable to stand?" may also provide some valuable information. Performing a gait analysis will yield some clues as to how the patient compensates during ambulation. Using plantar pressure plates can indicate load pressure differences between the feet. It is helpful if the gait analysis can be video-recorded and played back in slow motion to catch the subtle aspects of movement. Non Surgical Treatment Treatment is based on an estimate of how great the difference in leg length will be when the child grows up, Small differences (a half inch or less) do not need treatment. Differences of a half to one inch may require a lift inside the shoe.  how to increase height after 18 in 1 month Surgical Treatment Leg shortening is employed when LLD is severe and when a patient has already reached skeletal maturity. The actual surgery is called an osteotomy , which entails the removal of a small section of bone in the tibia (shinbone) and sometimes the fibula as well, resulting in the loss of around an inch in total height. Leg lengthening is a difficult third option that has traditionally had a high complication rate. Recently, results have improved somewhat with the emergence of a technique known as callotasis , in which only the outer portion of the bone (the cortex ) is cut, (i.e. a corticotomy ). This allows the bone to be more easily lengthened by an external fixation device that is attached to either side of the cut bone with pins through the skin. The ?ex-fix,' as it is sometimes called, is gradually adjusted by an orthopaedic surgeon, and healing can occur at the same time that the leg is being distracted , or lengthened over time. Unlike epiphysiodesis, leg lengthening procedures can be performed at almost any skeletal or chronological age. Overview
 Heel pain is a problem for many people. It makes standing and even walking around for long periods of time very uncomfortable. Several different conditions can lead to uncomfortable heels, but the most common culprit is plantar fasciitis. This is the inflammation and swelling of the plantar fascia, a tendon that runs along the sole of your foot and attaches to the bottom of the calcaneus, or heel bone. Repeated hard impacts or strain from overuse causes micro-tears to develop in the tendon, irritating it. The minor damage compounds over time and causes the tissue to swell and tighten, painfully pulling on the heel bone. Causes The most common cause of heel pain is a pull on the heel bone exerted by the muscles and ligaments (plantar fascia shown in illustration above) that support the arch of the foot. This is an overuse condition similar to bursitis of the shoulder or tennis elbow. Plantar fasciitis is typically very painful in the morning during the first few steps, after sitting and again at the end of the day. Symptoms Common symptoms, heel Spurs: the pain is usually worst on standing, particularly first thing in the morning when you get up. It is relatively common, though usually occurring in the over forty's age group. There are no visible features on the heel but a deep localised painful spot can be found in or around the middle of the sole of the heel. Although it is often associated with a spur of bone sticking out of the heel bone (heel spur syndrome), approximately ten per cent of the population have heel spurs without any pain. Heel Bursitis, pain can be felt at the back of the heel when the ankle joint is moved and there may be a swelling on both sides of the Achilles tendon. Or you may feel pain deep inside the heel when it makes contact with the ground. Heel Bumps, recognised as firm bumps on the back of the heel , they are often rubbed by shoes causing pain. Diagnosis A biomechanical exam by your podiatrist will help reveal these abnormalities and in turn resolve the cause of plantar fasciitis. By addressing this cause, the patient can be offered a podiatric long-term solution to his problem. Non Surgical Treatment Treatment of heel pain depends on its cause. Plantar fasciitis. Most doctors recommend a six- to eight-week program of conservative treatment, including temporary rest from sports that trigger the foot problem, stretching exercises, ice massage to the sole of the foot, footwear modifications, taping of the sole of the injured foot, and acetaminophen (Tylenol) or nonsteroidal anti-inflammatory drugs (NSAIDs), such as aspirin or ibuprofen (Advil, Motrin and others) for pain. If this conservative treatment doesn't help, your doctor may recommend that you wear a night splint or a short leg cast, or he or she may inject corticosteroid medication into the painful area. Surgery is rarely necessary and is not always successful. Heel spur. Conservative treatment includes the use of shoe supports (either a heel raise or a donut-shaped heel cushion) and a limited number of local corticosteroid injections (usually up to three per year). As in plantar fasciitis, surgery is a last resort. Calcaneal apophysitis. This condition usually goes away on its own. In the meantime, conservative treatment includes rest and the use of heel pads and heel cushions. Bursitis. Treatment is similar to the treatment of heel spurs. Changing the type of footwear may be essential. Surgical Treatment When a diagnosis of plantar fasciitis is made early, most patients respond to conservative treatment and don?t require surgical intervention. Often, when there is a secondary diagnosis contributing to your pain, such as an entrapped nerve, and you are non-responsive to conservative care, surgery may be considered. Dr. Talarico will discuss all options and which approach would be the most beneficial for your condition. how to get rid of heel spurs Prevention  The following steps will help prevent plantar fasciitis or help keep the condition from getting worse if you already have it. The primary treatment is rest. Cold packs application to the area for 20 minutes several times a day or after activities give some relief. Over-the-counter pain medications can help manage the pain, consult your healthcare professional. Shoes should be well cushioned, especially in the midsole area, and should have the appropriate arch support. Some will benefit from an orthotic shoe insert, such as a rubber heel pad for cushioning. Orthotics should be used in both shoes, even if only one foot hurts. Going barefoot or wearing slipper puts stress on your feet. Put on supportive shoes as soon as you get out of bed. Calf stretches and stretches using a towel (place the towel under the ball of your feet and pull gently the towel toward you and hold a few seconds) several times a day, especially when first getting up in the morning. Stretching the Achilles tendon at the back of the heel is especially important before sports, but it is helpful for nonathletes as well. Increasing your exercise levels gradually. Staying at a healthy weight. Surgery is very rarely required. Overview
 Mortons Neuroma is a common painful condition involving compression of nerves between the long bones of the forefoot just before they enter the toes. Commonly this involves the 3rd and 4th toes, however may affect the 2nd and 3rd toes. Repeated trauma or compression of these nerves causes the nerves to swell and thicken causing a Morton's neuroma to develop. Mortons Neuroma is a common painful condition involving compression of nerves between the long bones of the forefoot just before they enter the toes. Commonly this involves the 3rd and 4th toes, however may affect the 2nd and 3rd toes. Repeated trauma or compression of these nerves causes the nerves to swell and thicken causing a Morton's neuroma to develop.Causes Morton's neuroma is an inflammation caused by a buildup of fibrous tissue on the outer coating of nerves. This fibrous buildup is a reaction to the irritation resulting from nearby bones and ligaments rubbing against the nerves. Irritation can be caused by Wearing shoes that are too tight. Wearing shoes that place the foot in an awkward position, such as high heels. A foot that is mechanically unstable. Repetitive trauma to the foot such as from sports activities like tennis, basketball, and running. Trauma to the foot caused by an injury such as a sprain or fracture. It is unusual for more than one Morton's neuroma to occur on one foot at the same time. It is rare for Morton's neuroma to occur on both feet at the same time. Symptoms Morton's neuroma can cause a very painful burning or sharp pain in your foot that feels worse when you walk. It may feel like a small lump inside the ball of your foot. It is usually between the third and fourth toes, but it can also be between other toes. Diagnosis Morton?s neuroma can be identified during a physical exam, after pressing on the bottom of the foot. This maneuver usually reproduces the patient?s pain. MRI and ultrasound are imaging studiesthat can demonstrate the presence of the neuroma. An x-ray may also be ordered to make sure no other issues exist in the foot. A local anesthetic injection along the neuroma may temporarily abolish the pain, and help confirm the diagnosis. Non Surgical Treatment Treatment for Morton's neuroma may depend on several factors, including the severity of symptoms and how long they have been present. The earlier on the condition is diagnosed, the less likely surgery is required. Doctors will usually recommend self-help measures first. These may include resting the foot, massaging the foot and affected toes. Using an ice pack on the affected area (skin should not be directly exposed to ice, the ice should be in a container or wrapped in something) Changing footwear, wearing wide-toed shoes, or flat (non high-heeled) shoes. Trying arch supports (orthotic devices). A type of padding that supports the arch of the foot, removing pressure from the nerve. The doctor may recommend a custom-made, individually designed shoe-insert, molded to fit the contours of the patient's foot. There are several OTC (over the counter, non-prescription) metatarsal pads or bars available which can be placed over the neuroma. Taking over-the-counter, non-prescription painkilling medications. Modifying activities, avoiding activities which put repetitive pressure on the neuroma until the condition improves. Bodyweight management,if the patient is obese the doctor may advise him/her to lose weight. A significant number of obese patients with foot problems, such as flat feet, who successfully lose weight experience considerable improvement of symptoms.  Surgical Treatment For severe or persistent pain, you may need surgery to remove the neuroma. Once the nerve is gone, you permanently lose feeling in the affected area. One alternative to surgery is to undergo neurolysis injections. These use chemical agents to block pain signals. Another alternative is to take a prescription pain reliever that alleviates nerve pain. Prevention Women, particularly those who wear tight shoes, are at greatest risk for Morton?s neuroma. The best way to prevent the condition is to wear shoes with wide toe boxes. Tight, pointed shoes squeeze bones, ligaments, muscles and nerves. High heels may worsen the problem by shifting your weight forward. Over time, this combination can cause the nerves to swell and become painful. There are not one but two different kinds of leg length discrepancies, congenital and acquired. Congenital means you are born with it. One leg is structurally shorter in comparison to the other. As a result of developmental stages of aging, the brain picks up on the step pattern and recognizes some difference. Our bodies usually adapts by tilting one shoulder to the "short" side. A difference of less than a quarter inch isn't very uncommon, require Shoe Lifts to compensate and mostly does not have a serious effect over a lifetime.
 Leg length inequality goes typically undiagnosed on a daily basis, however this problem is simply corrected, and can reduce many incidents of back ache. Treatment for leg length inequality usually consists of Shoe Lifts . They are affordable, often costing less than twenty dollars, compared to a custom orthotic of $200 if not more. When the amount of leg length inequality begins to exceed half an inch, a whole sole lift is generally the better choice than a heel lift. This prevents the foot from being unnecessarily stressed in an abnormal position. Mid back pain is the most prevalent condition impacting men and women today. Over 80 million people have problems with back pain at some point in their life. It is a problem which costs employers vast amounts of money annually due to lost time and production. New and more effective treatment solutions are continually sought after in the hope of reducing the economic impact this issue causes.  People from all corners of the world suffer the pain of foot ache due to leg length discrepancy. In these situations Shoe Lifts might be of very helpful. The lifts are capable of decreasing any discomfort in the feet. Shoe Lifts are recommended by numerous specialist orthopaedic orthopedists. So that they can support the body in a well-balanced fashion, your feet have got a critical task to play. In spite of that, it can be the most neglected zone in the human body. Many people have flat-feet meaning there is unequal force exerted on the feet. This causes other parts of the body including knees, ankles and backs to be affected too. Shoe Lifts guarantee that appropriate posture and balance are restored.  Overview A calcaneal spur (or heel spur) is a small osteophyte (bone spur) located on the calcaneus (heel bone). Calcaneal spurs are typically detected by a radiological examination (X-ray). When a foot bone is exposed to constant stress, calcium deposits build up on the bottom of the heel bone. Generally, this has no effect on a person's daily life. However, repeated damage can cause these deposits to pile up on each other,causing a spur-shaped deformity, called a calcaneal (or heel) spur. Obese people, flatfooted people, and women who constantly wear high-heeled shoes are most susceptible to heel spurs. An inferior calcaneal spur is located on the inferior aspect of the calcaneus and is typically a response to plantar fasciitis over a period, but may also be associated with ankylosing spondylitis (typically in children). A posterior calcaneal spur develops on the back of the heel at the insertion of the Achilles tendon. An inferior calcaneal spur consists of a calcification of the calcaneus, which lies superior to the plantar fascia at the insertion of the plantar fascia. A posterior calcaneal spur is often large and palpable through the skin and may need to be removed as part of the treatment of insertional Achilles tendonitis. These are also generally visible to the naked eye. Causes When the Plantar Fascia is allowed to rest during sleep or long periods of inactivity, the fascia tightens and shortens. When you first stand up after resting, the fascia is forced to stretch very quickly causing micro-tears in the tissue. This is why the first steps in the morning are so exquisitely painful. Heel spurs are more likely to happen if you suffer from over-pronation (walking with a rolling gait) you stand or walk on rigid surfaces for long periods, you are above ideal weight or during pregnancy, you have stiff muscles in your calves.  Symptoms With heel spurs, people often talk about a dull ache which is felt most of the time with episodes of a sharp pain in the center of the heel or on the inside margin of the heel. Often the pain is worse on first rising in the morning and after rest and is aggravated by prolonged weight bearing and thin-soled shoes. Diagnosis Your doctor will review your medical history and examine your foot. X-rays are used to identify the location and size of the heel spur. Non Surgical Treatment Rest won?t help you in case of pain from the heel spur. When you get up after sleeping for some time, the pain may get worse. The pain worsens after a period of rest. You will feel pain because the plantar fascia elongates during working which stresses the heel. It is important to see a doctor if you are having consistent pain in you heel. The doctors may advise few or all of the conservative treatments, stretching exercises, shoe recommendations, shoe inserts or orthotic devices, physical therapy, taping or strapping to rest stressed muscles and tendons. There are some over-the-counter medicines available for treatment of heel pain. Acetaminophen (Tylenol), ibuprofen (Advil), or naproxen (Aleve) are some such medicines which can help you to get relief from the pain. In case of biomechanical imbalances causing the pain, a functional orthotic device can help you to get relief. Your doctor may also advise a corticosteroid injection for eliminating the inflammation. Surgical Treatment Have surgery if no other treatments work. Before performing surgery, doctors usually give home treatments and improved footwear about a year to work. When nothing else eases the pain, here's what you need to know about surgical options. Instep plantar fasciotomy. Doctors remove part of the plantar fascia to ease pressure on the nerves in your foot. Endoscopy. This surgery performs the same function as an instep plantar fasciotomy but uses smaller incisions so that you'll heal faster. However, endoscopy has a higher rate of nerve damage, so consider this before you opt for this option. Be prepared to wear a below-the-knee walking cast to ease the pain of surgery and to speed the healing process. These casts, or "boots," usually work better than crutches to speed up your recovery time. Prevention Use orthotic inserts. You can purchase orthotics over the counter, or you can have orthotics specially fitted by your podiatrist. Try 1 of these options. Heel cups. These inserts will help to align the bones in your foot and to cushion your heel. Check your skin for blisters when you first start using heel cups. Also, your feet may sweat more with a heel cup, so change your socks and shoes often. Insoles. While you can pick up generic insoles at a drugstore, you may have more luck if you go to a store that sells athletic shoes. Push on the arch to make sure that it doesn't collapse. If your insoles help but could use a little work, you can take them to a podiatrist to get them customized. Custom orthotics. A podiatrist can make a cast of your foot and provide you with custom-made orthotics. These may be more expensive, but they are made of materials specifically designed for your needs, and they can last up to 5 years if your podiatrist refurbishes them every 1 or 2 years. To find a podiatrist near you, look at the Web page for the American Academy of Podiatric Sports Medicine. Dynamic Insoles. Lack of elasticity in plantar fascia in the foot is for most people the real problem. If there is poor elasticity in the lengthwise tendons in the foot (plantar fascia) in relation to a person's general condition, only a small additional strain is required for the pull on the tendons to cause damage to the tissues connecting the tendons to the heel bone. This will generate an inflamed condition called Plantar Fasciitis.  Overview A heel spur is a hook that can form on the calcaneus (heel bone) and can also be related to plantar fasciitis (inflammation of the tissue in the foot?s arch). People who have plantar fasciitis often develop heel spurs. Middle-aged men and women are more prone to heels spurs, but all age groups can be afflicted. Heel spurs can be found through an x-ray, revealing a protruding hook where the plantar fascia is located. Causes Bone spurs form in the feet in response to tight ligaments, to activities such as dancing and running that put stress on the feet, and to pressure from being overweight or from poorly fitting shoes. For example, the long ligament on the bottom of the foot (plantar fascia) can become stressed or tight and pull on the heel, causing the ligament to become inflamed (plantar fasciitis). As the bone tries to mend itself, a bone spur can form on the bottom of the heel (known as a ?heel spur?). Pressure at the back of the heel from frequently wearing shoes that are too tight can cause a bone spur on the back of the heel. This is sometimes called a ?pump bump,? because it is often seen in women who wear high heels.  Symptoms Heel spurs often do not show any symptoms. If you have intermittent or chronic pain when you walk, run or jog, it may be heel spur. There will be inflammation the point where spur formation happens. The pain is caused by soft tissue injury in the heel. Patients often describe the pain as a pin or knife sticking to the heel. The pain is more specially in the morning when the patient stands up for the first time. Diagnosis A Diagnosis of Heel Spur Syndrome is a very common reason for having heel pain. Heel pain may be due to other types of conditions such as tendonitis, Haglund's Deformity, Stress Fracture, Tarsal Tunnel Syndrome, or low back problems. A more common condition in children is Sever's Disease. The diagnosis is usually made with a combination of x-ray examination and symptoms. Non Surgical Treatment The first line of treatment for Heel Spur is to avoid the activities and positions that cause the pain. A physician can evaluate your foot with an X-ray to diagnose Heel Spur and determine a course of treatment. This condition can often be treated by non-surgical means; however in severe cases surgery may be necessary to relieve the pain. The most common surgical procedures treat the soft tissues around the Heel Spur, often a tarsal tunnel release or a plantar fascia release. Injections for heel spurs are sometimes controversial as steroids may cause heel pad atrophy or damage the plantar fascia. Surgical Treatment Heel spur surgery should only be considered after less invasive treatment methods have been explored and ruled insufficient. The traditional surgical approach to treating heel spurs requires a scalpel cut to the bottom of the food which allows the surgeon to access the bone spur. Endoscopic plantar fasciotomies (EPF) involve one or two small incisions in the foot which allow the surgeon to access and operate on the bone spur endoscopically. Taking a surgical approach to heel spur treatment is a topic to explore with a foot and ankle specialist. Prevention Heel Spur symptoms can be prevented from returning by wearing proper shoes and using customized orthotics and insoles to relieve pressure. It is important to perform your exercises to help keep your foot stretched and relaxed. Overview
Bursae (two or more bursa) are small, fluid-filled sacs that cushion the bones, tendons and muscles surrounding your joints. They contain a lubricating fluid that reduces friction, allowing tissues in the body to glide past each other smoothly. Imagine the bursa as a protective layer that helps keep a tendon or muscle from fraying or getting aggravated as it eases over a bone or around a corner. Bursitis is a condition that occurs when a bursa becomes inflamed: irritated, red and filled with more fluid than normal. Causes Bursitis can develop for several reasons, including repetitively engaging in the same motion, or example, lifting objects above your head for work. Putting a lot of pressure on a bursa for an extended period of time. Leaning on your elbows or kneeling (for example, to lay carpet) can cause bursitis in the elbows or knees. If you sit for long periods of time, especially on hard surfaces, you may develop bursitis in your hip. Wearing shoes with a stiff back that rubs against the back of the ankle can cause Achilles tendon bursitis. Trauma. The bursae at the knee and elbow are close to the surface of the skin, and if you fall directly on your elbow or the knee, you can rupture, injure or puncture a bursa. Infection. Known as septic bursitis, it?s the result of bacteria infecting a bursa. It can occur from an infection traveling from another site or following an accident that ruptures the bursa. Even scraping the skin on your elbow or getting a mosquito bite that breaks the skin near the olecranon bursa (near the elbow) can lead to bursitis. Other joint disorders, such as rheumatoid arthritis, osteoarthritis and gout, or health conditions. Symptoms Posterior heel pain is the chief complaint in individuals with calcaneal bursitis. Patients may report limping caused by the posterior heel pain. Some individuals may also report an obvious swelling (eg, a pump bump, a term that presumably comes from the swelling's association with high-heeled shoes or pumps). The condition may be unilateral or bilateral. Symptoms are often worse when the patient first begins an activity after rest. Diagnosis Diagnosis is first by clinical suspicion of symptoms. This can be mistaken for gout or infection especially in the big toe region. A diagnosis of bursitis is usually used in combination of the underlying cause, for instance a bunion deformity, Haglund's deformity, or Heel Spur Syndrome. Many times the cause needs to be addressed to rid the problem of bursitis. Non Surgical Treatment Treatment consists of anti-inflammatory therapy with the use of ice, short term non steroidal therapy including ibuprofen and naproxen and selective use of cortisone injections. Cortisone injections have been shown to be a highly effective anti-inflammatory measure for relieving foot and ankle pain. Care must always be taken by the physician to insure that the injection is administered into the bursal sac and not the Achilles tendon which can cause tendon injury. Treatment also consists of the use of heel lifts or the temporary use of a shoe with a low heel. The heel lift decreases the mechanical load on the Achilles tendon. Gentle stretching of the Achilles tendon, the possible use of a splint that is worn at night as well as physical therapy as directed by your physician can be employed. Temporary activity limitations for fitness must be incorporated into the treatment plan. Any weight bearing activity for exercise that actively lifts your heel off of the ground including running, walking stair stepper will interfere with effective conservative care. Low impact activity including biking and pool tend to be safe exercises during your recovery. Surgical Treatment Surgery to remove the damaged bursa may be performed in extreme cases. If the bursitis is caused by an infection, then additional treatment is needed. Septic bursitis is caused by the presence of a pus-forming organism, usually staphylococcus aureus. This is confirmed by examining a sample of the fluid in the bursa and requires treatment with antibiotics taken by mouth, injected into a muscle or into a vein (intravenously). The bursa will also need to be drained by needle two or three times over the first week of treatment. When a patient has such a serious infection, there may be underlying causes. There could be undiscovered diabetes, or an inefficient immune system caused by human immunodeficiency virus infection (HIV).  Overview OverviewA hammertoes can be flexible or rigid. Hammertoes often start out flexible and become rigid over time as your toe becomes accustomed to its crooked position. Flexible hammertoes are less serious than rigid hammertoes, as they can be easily diagnosed and treated in Hammer toe their initial stages. Flexible hammertoes are named as such because your affected toe still possesses some degree of movement. Causes Hammertoe commonly develops because of structural changes that take place over time in the muscles and tendons that bend the toes. People with certain medical conditions, such as diabetes, are at risk for developing hammertoe. It can be an inherited condition for some people. Other causes include trauma and wearing shoes that are too tight, narrow, or have high heels. The toe next to the big toe (second toe) is most frequently affected by hammertoe.  Symptoms SymptomsThe most common symptoms of hammertoes include. The toe is bent upward at the middle toe joint, so that the top of this joint rubs against the top of the shoe. The remainder of the toe is bent downward. Pain upon pressure at the top of the bent toe from footwear. The formation of corns on the top of the joint. Redness and swelling at the joint contracture. Restricted or painful motion of the toe joint. Pain in the ball of the foot at the base of the affected toe. This occurs because the contracted digit puts pressure on the metatarsal head creating callouse and pressure on the ball of the foot. Diagnosis Your healthcare provider will examine your foot, checking for redness, swelling, corns, and calluses. Your provider will also measure the flexibility of your toes and test how much feeling you have in your toes. You may have blood tests to check for arthritis, diabetes, and infection. Non Surgical Treatment Inserts in your shoes can be used to help relieve pressure on the toes from the deformity. Splints/Straps. These can be used to help re-align and stretch your toes and correct the muscle imbalance and tendon shortening. One of the most common types are toe stretchers like the yogatoe. Chiropody. A chiropodist can remove calluses or corns, areas of hard skin that have formed to make the foot more comfortable.Steroid injections can help to reduce pain and inflammation. Surgical Treatment Sometimes, if the deformity is severe enough or surgical modification is needed, the toe bones may be fused so that the toe does not bend. Buried wires are used to allow for the fusion to heal, and they remain in place after healing. Your skin is closed with fine sutures, which are typically removed seven to ten days after surgery. A dressing is used to help keep your toes in their new position. Dressings should not get wet or be removed. After surgery, your doctor may prescribe pain relievers, typically for the initial four to seven days. Most people heal completely within one month of surgery, with few complications, if any. Crutches or a cane may be needed to help you keep weight off your affected foot, depending on the procedure. Occasionally, patients receive a special post-op shoe or a walking boot that is to be worn during the healing process. Most people are able to shower normally after surgery, but must protect the dressing from getting wet. Many patients are allowed to resume driving within one week after the procedure, but care needs to be taken.  Prevention PreventionAvoid wearing shoes that are too short or narrow. Check children's shoe sizes often, especially during periods of fast growth. If you have hammer toe, call for an appointment with your health care provider. If you develop thick blisters or corns on your toes, if your pain gets worse, if you have difficulty walking call for an appointment with your health care provider.
Overview
 Bunions are common but they can be misdiagnosed. We sometimes assume that any lump at the bottom of the big toe is a bunion. But as the Latin name (hallux valgus) suggests, the hallmark of a bunion is what happens to the toe itself (the hallux) rather than to the joint at its base. In bunions, the toe veers off in a valgus direction, that is, away from the midline. An outcrop of extra bone, or osteophyte, develops as the body tries to protect the exposed surface of the warped first metatarsophalangeal joint (MTP); a fluid-filled sac, or bursa, may also form, which often becomes inflamed. Foot experts are still not entirely agreed about what causes bunions. Genetics and lax ligaments are both implicated; the role of footwear is less clear. All bunion conversations seem to involve someone stating that barefoot tribes people don?t get bunions. This is not true. Bunions are common but they can be misdiagnosed. We sometimes assume that any lump at the bottom of the big toe is a bunion. But as the Latin name (hallux valgus) suggests, the hallmark of a bunion is what happens to the toe itself (the hallux) rather than to the joint at its base. In bunions, the toe veers off in a valgus direction, that is, away from the midline. An outcrop of extra bone, or osteophyte, develops as the body tries to protect the exposed surface of the warped first metatarsophalangeal joint (MTP); a fluid-filled sac, or bursa, may also form, which often becomes inflamed. Foot experts are still not entirely agreed about what causes bunions. Genetics and lax ligaments are both implicated; the role of footwear is less clear. All bunion conversations seem to involve someone stating that barefoot tribes people don?t get bunions. This is not true.Causes Inflammatory joint diseases. Those who suffer from rheumatoid and psoriatic arthritis are at risk for bunions, although many times, those who suffer from bunions will mistakenly attribute the soreness in their feet to arthritis. Genetic and neuromuscular factors. Individuals with Down?s Syndrome are believed to be more prone to developing bunions; therefore, the gait and feet of such patients should be examined carefully and regularly so that any problems can be caught and treated early. Similarly, individuals of any age who have been diagnosed with Ehlers-Danlos or Marfan?s Syndrome, have also been shown to have a higher than average occurrence of bunions. Limb inequality. Individuals who have legs of unequal length often suffer from bunions on the longer limb due to the irregular mechanics of their walking or running gait. Symptoms The main problem is usually the pressure of the shoe over the bony prominence, which causes discomfort or pain. Sometimes the skin over the lump becomes red, blistered or infected. The foot may become so broad that it is difficult to get wide enough shoes. The big toe sometimes tilts over so much that it rubs on the second toe, or pushes it up out of place so it presses on the shoe. Also, the big toe does not work as well with a bunion, and the other toes have to take more of the weight of the body as you walk. This can cause pain under the ball of the foot ("metatarsalgia"). Sometimes arthritis develops in the deformed joint, causing pain in the joint. Diagnosis A thorough medical history and physical exam by a physician is necessary for the proper diagnosis of bunions and other foot conditions. X-rays can help confirm the diagnosis by showing the bone displacement, joint swelling, and, in some cases, the overgrowth of bone that characterizes bunions. Doctors also will consider the possibility that the joint pain is caused by or complicated by Arthritis, which causes destruction of the cartilage of the joint. Gout, which causes the accumulation of uric acid crystals in the joint. Tiny fractures of a bone in the foot or stress fractures. Infection. Your doctor may order additional tests to rule out these possibilities. Non Surgical Treatment Bunions may be treated conservatively with changes in shoe gear, different orthotics (accommodative padding and shielding), rest, ice and medications. These sorts of treatments address symptoms more than they correct the actual deformity. Surgery, by an orthopedic surgeon or a podiatric surgeon, may be necessary if discomfort is severe enough or when correction of the deformity is desired. Orthotics are splints or regulators while conservative measures include various footwear like gelled toe spacers, bunion toes separators, bunion regulators, bunion splints and bunion cushions. There are a variety of available orthotics (or orthoses) including over-the-counter or off-the-shelf commercial products and as necessary, custom-molded orthotics that are generally prescribed medical devices. 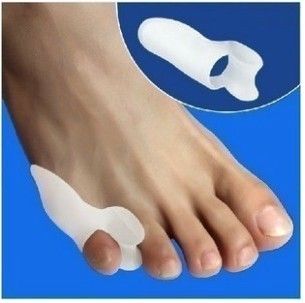 Surgical Treatment Surgical options, such as a bunionectomy, can remove the bunion and realign the toe. There are several types of surgeries to fix the bunion. The type of bunion you have along with other factors such as the degree of severity and underlying cause of the bunion will determine which approach would be most beneficial for you. Prevention If these exercises cause pain, don't overdo them. Go as far as you can without causing pain that persists. This first exercise should not cause pain, but is great for stimulating blood and lymphatic circulation. Do it as often as you can every day. Only do this exercise after confirming it is OK with your doctor. Lie on your back and lift up your legs above you. Wiggle your toes and feet. Eventually you may be able to rapidly shake your feet for a minute at a time. Use your fingers to pull your big toe into proper alignment. Stretch your big toe and the rest of your toes. Curl them under for 10 seconds, then relax and let them point straight ahead for 10 seconds. Repeat several times. Do this at least once a day, and preferably several times. Flex your toes by pressing them against the floor or a wall until they are bent back. Hold them for 10 seconds, then release. Repeat several times. Grip with your toes. Practice picking up an article of clothing with your toes, dropping it, and then picking it up again. Warm water. Soak your feet for 20 minutes in a bowl of warm water. Try doing the foot exercises while soaking, and also relax and rest your feet. Epsom salts. Add it to your warm foot bath soak. |
