|
Overview
Foot types can be divided into three major groups: the flat foot (Pes Planus), the high arched foot (Pes Valgus) and the normal to low arched foot. A true 'flat foot' is very rare. In fact, less than 5% of the population have flat feet i.e. a foot with no arch present whatsoever and the entire bottom surface of the foot being flat on the ground. About 5-10% of people have a high arched foot. The majority of the population have a normal to low arch. Even though the arches appear to be normal most of us suffer from over-pronation during walking, running and standing, due to the hard, flat unnatural surfaces we walk on, combined with wearing unsupportive footwear. With every step we take the arches flatten and the ankles roll inwards. Pronation itself is not wrong because we need to pronate and supinate as part of our natural gait cycle. Pronation (rolling in) acts as a shock-absorbing mechanism and supination (rolling out) helps to propel our feet forward. Over-pronation occurs when the foot pronates too deep and for too long, not allowing the foot to 'recover' and supinate. Over-pronation hampers our natural walking pattern. It causes an imbalance and leads to wear and tear in several parts of the body with every step we take.  Causes Flat feet don't automatically mean you have a problem. The problem can be divided into a flexible flat foot or rigid flat foot. The rigid flat foot is one that does not change shape when the foot becomes weight bearing. i.e. it does not go through the excessive motion of pronation. Generally speaking this foot does not provide too many problems. The flexible flat foot is the type that when it becomes weight bearing the foot and ankle tends to roll in (pronates) too far. This type of person will often say I have great arches but when I stand up much of this arch disappears as the foot excessively pronates When the foot is excessively pronating and causing problems like sore ankles, feet or knees when standing or exercising then arch support is extremely important to restore the foot structure. Symptoms Overpronation can lead to injuries and pain in the foot, ankle, knee, or hip. Overpronation puts extra stress on all the bones in the feet. The repeated stress on the knees, shins, thighs, and pelvis puts additional stress on the muscles, tendons, and ligaments of the lower leg. This can put the knee, hip, and back out of alignment, and it can become very painful. Diagnosis A quick way to see if you over-pronate is to look for these signs. While standing straight with bare feet on the floor, look so see if the inside of your arch or sole touches the floor. Take a look at your hiking or running shoes; look for wear on the inside of the sole. Wet your feet and walk on a surface that will show the foot mark. If you have a neutral foot you should see your heel connected to the ball of your foot by a mark roughly half of width of your sole. If you over-pronate you will see greater than half and up to the full width of your sole.  Non Surgical Treatment The following exercises help retrain the foot and ankle complex to correct overpronation. Exercises may be performed while wearing shoes, or for an even greater challenge, in bare feet. Duck Stand. This exercise is designed to prepare for the more dynamic BT exercises ahead by waking up the gluteal muscles and teaching clients how the gluteal muscles control the degree of foot pronation. For example, when the glutes contract concentrically, they rotate the leg outward. As the leg rotates outward, the arch of the foot raises (i.e., supinates). Stand beside the BT with both heels together and feet turned outward. (Note: As you progress, perform this exercise while standing on the BT.) Try to rotate legs outward by tightening buttock muscles while tilting pelvis under. As legs rotate outward, arches of the feet raise up out of pronation. Hold position for 30 seconds. Big Toe Pushdowns. This exercise is designed to strengthen the muscle of the big toe that holds up the arch of the foot (i.e., flexor hallucis longus muscle). This stops the foot from overpronating. Stand on top of the BT dome with feet facing forward. Use gluteal muscles to raise the arches of the feet (see previous exercise - "Duck Stand"). Keep arches raised while pushing down big toe into the BT. While pushing down, tension build in the arch on the underside of their foot should be felt. Hold position for 15 seconds. Surgical Treatment Subtalar Arthroereisis. The ankle and hindfoot bones/midfoot bones around the joint are fused, locking the bones in place and preventing all joint motion. This may also be done in combination with fusion at other joints. This is a very aggressive option usually reserved for extreme cases where no joint flexibility is present and/or the patient has severe arthritic changes in the joint. Overview
Pain in the heel of a child's foot, typically brought on by some form of injury or trauma, is sometimes Sever's Disease. The disease often mimics Achilles tendonitis, an inflammation of the tendon attached to the back of the heel. A tight Achilles tendon may contribute to Sever's Disease by pulling excessively on the growth plate of the heel bone. This condition is most common in younger children and is frequently seen in the active soccer, football or baseball player. Sport shoes with cleats are also known to aggravate the condition. Treatment includes calf muscle stretching exercises, heel cushions in the shoes, and/or anti-inflammatory medications. Consult your physician before taking any medications. Causes Sever?s disease is common, and typically occurs during a child?s growth spurt, which can occur between the ages of 10 and 15 in boys and between the ages of 8 and 13 in girls. Feet tend to grow more quickly than other parts of the body, and in most kids the heel has finished growing by the age of 15. Being active in sports or participating in an activity that requires standing for long periods can increase the risk of developing Sever?s disease. In some cases, Sever?s disease first becomes apparent after a child begins a new sport, or when a new sports season starts. Sports that are commonly associated with Sever?s disease include track, basketball, soccer, and gymnastics. Children who are overweight or obese are also at a greater risk of developing this condition. Certain foot problems can also increase the risk, including. Over pronating. Kids who over pronate (roll the foot inward) when walking may develop Sever?s disease. Flat foot or high arch. An arch that is too high or too low can put more stress on the foot and the heel, and increase the risk of Sever?s disease. Short leg. Children who have one leg that is shorter than the other may experience Sever?s disease in the foot of the shorter leg because that foot is under more stress when walking. Symptoms Unilateral or bilateral heel pain. Heel pain during physical exercise, especially activities that require running or jumping. Increased pain level after exercise. A tender swelling or bulge on the heel that is painful on touch. Limping. Calf muscle stiffness first thing in the morning. Diagnosis Children or adolescents who are experiencing pain and discomfort in their feet should be evaluated by a physician. In some cases, no imaging tests are needed to diagnose Sever?s disease. A podiatrist or other healthcare professional may choose to order an x-ray or imaging study, however, to ensure that there is no other cause for the pain, such as a fracture. Sever?s disease will not show any findings on an x-ray because it affects cartilage. Non Surgical Treatment The primary method of treating Sever?s disease is taking time off from sports and other physical activities to alleviate the pressure on the heel bone. During the healing period, your child?s doctor may also recommend physical therapy or any type of exercise that involves stretching and strengthen leg muscles and tendons. Wrapping ice in a towel and placing it under the child?s heel will also help to alleviate and reduce pain and swelling. Exercise Exercises that help to stretch the calf muscles and hamstrings are effective at treating Sever's disease. An exercise known as foot curling, in which the foot is pointed away from the body, then curled toward the body in order to help stretch the muscles, has also proven to be very effective at treating Sever's disease. The curling exercise should be done in sets of 10 or 20 repetitions, and repeated several times throughout the day. Overview
Flat feet are a common condition. In infants and toddlers, the longitudinal arch is not developed and flat feet are normal. Most feet are flexible and an arch appears when the person stands on his or her toes. The arch develops in childhood, and by adulthood most people have developed normal arches. Most flat feet usually do not cause pain or other problems. Flat feet may be associated with pronation, a leaning inward of the ankle bones toward the center line. Shoes of children who pronate, when placed side by side, will lean toward each other (after they have been worn long enough for the foot position to remodel their shape). Foot pain, ankle pain or lower leg pain, especially in children, may be a result of flat feet and should be evaluated.  Causes Having low or no arches is normal for some people. In these cases, flat feet are usually inherited and the feet are fairly flexible. Occasionally, flat feet can be caused by an abnormality that develops in the womb, such as a problem with a joint or where two or more bones are fused together. This is known as tarsal coalition and results in the feet being flat and stiff. Flat feet that develop in later life can be caused by a condition that affects the joints, such as arthritis, or an injury to a muscle, tendon or joint in the foot. Symptoms Go to a podiatrist at the first sign of symptoms. Besides pain on the bottom of the foot, additional symptoms may include burning sensation in arch, difficulty standing on tiptoes, inflammation, more pain after sleeping or resting, redness, heat, localized pain in the ball of the foot, sharp or shooting pain in the toes, pain that increases when toes are flexed, tingling or numbness in the toes, aching, pain that increases when walking barefoot, pain that increases when walking on hard surfaces, pain the increases when standing (putting weight on your feet) or moving around and decreases when immobile, skin Lesions, it?s important to get a proper diagnosis and treatment plan. Let?s go over the possible causes of the pain. Diagnosis A professional therapist may use tinels test to diagnose tarsal tunnel syndrome. This involves tapping the nerve just behind the medial malleolus or bony bit of the ankle with a rubber hammer. Pain indicates a positive test. Sometimes it is initially mistaken for plantar fasciitis which also causes pain from the inside heel and throughout the arch of the foot. Neural symptoms (such as tingling or numbness) as well as the location of tenderness when touching the area should help to easily distinguish between the conditions. Non Surgical Treatment Changes in shoes to include more supportive sport shoes or walking shoes that have a softer footbed. Oral anti-inflammatories including over-the-counter medications such as Brufen can help acute flare ups. Prescription strength anti-inflammatories prescribed by your GP or doctor. Prescription Transdermal Verapamil gel, which can reduce scar tissue. Anti-inflammatory injections (cortisone-type medications) into the mass and surrounding areas to decrease the inflammation. Stretching exercises, this may worsen the problem as it stretches the area of tear. Massage including tennis ball orfrozen water bottle massage of the arch - as with stretching this may worsen the problem. Taping or strapping of the foot, arch or ankle to reduce the pressure on the plantar fascia. Long term conservative treatment should include custom moulded functional orthotics. The orthotics should have an accommodation for the plantar fibroma, this is probably the best conservative treatment for plantar fibroma.  Surgical Treatment A procedure that involves placing a metallic implant (most commonly) at the junction where the foot meets the ankle. This device causes the physical blockade that prevent the collapse. It is a procedure that is only indicated for mobile feet, and should not be used with rigid flat feet. Dr. Blitz finds this procedure better for younger patients with flexible flat feet where the bone alignment is still developing so that the foot can adapt to function in a better aligned position. Prevention Drink plenty of water before, during and after your workout. Dehydration is a common cause of muscle cramps, according to MayoClinic.com. If your workouts are long and strenuous, drink a carbohydrate-based electrolyte beverage too. Warm up the muscles of your feet before you work out. A simple exercise is to write the letters of the alphabet with your toes. Perform the warm up with bare feet and exaggerate the movements to challenge your muscles. Wear properly fitted shoes. Visit a sporting goods store and get your feet and arches measured. Ask for help selecting a pair of shoes to fit your workout. For instance, if you play soccer, you need cleats, not running shoes. Take a break. Cramps can be your body's way of telling you you're exercising too much, according to MayoClinic.com. Rest for a few days, then resume exercise and see if you can complete a workout without arch cramps. Stretch. At the end of your workout, perform a few stretching exercises to keep your muscles from tightening and cramping. Sit down, lean over and grasp your toes. Pull the toes toward your body until you feel tension in the arch of your foot. Hold the stretch for 20 to 30 seconds, then repeat on the opposite side. Another easy way to stretch your arch is to put a towel on the floor, curl your toes around it and pull it toward your body. Stretching Exercises Calf Raises. Strengthens the tendons in your heels and calf muscles, which support your arch. Raise up on the balls of your feet as high as possible. Slowly lower down. Do three sets of 10 reps. Progress to doing the raises on stairs (with heels hanging off), and then to single-leg raises. Step Stretch. Improves flexibility in your Achilles tendon and calf-when these areas become tight, the arch gets painfully overloaded. Stand at the edge of a step, toes on step, heels hanging off. Lower your heels down, past the step, then raise back up to the start position. Do three sets of 10 reps. Doming. Works the arch muscles and the tibialis posterior (in the calf and foot) to control excess pronation. While standing, press your toes downward into the ground while keeping the heel planted, so that your foot forms an arch (or dome). Release, and do three sets of 10 reps on each foot. Toe Spread and Squeeze. Targets the interossei muscles of the foot, which support the arch. While sitting, loop a small resistance band around your toes. Spread toes; release. Then place a toe separator (used at nail salons) in between toes. Squeeze toes in; release. Do three sets of 10 reps of each exercise on both feet. Towel Curls. Works the toe-flexor muscles that run along your arch to increase overall foot strength. Lay a small hand towel on the floor, and place one foot on the towel. Using just your toes, scrunch the towel toward you, hold, then slowly push the towel away from you back to start position. Do three sets of 10 reps on each foot.
Overview
 Pain of the Achilles tendon commonly affects both competitive and recreational athletes, and the sedentary. The largest tendon in the body, the Achilles tendon, endures strain and risks rupture from running, jumping, and sudden acceleration or deceleration. Overuse, vascular diseases, neuropathy, and rheumatologic diseases may cause tendon degeneration. The hallmarks of Achilles tendon problems seem to be damaged, weak, inelastic tissue. Causes An Achilles tendon injury might be caused by several factors. Overuse. Stepping up your level of physical activity too quickly. Wearing high heels, which increases the stress on the tendon. Problems with the feet, an Achilles tendon injury can result from flat feet, also known as fallen arches or overpronation. In this condition, the impact of a step causes the arch of your foot to collapse, stretching the muscles and tendons. Muscles or tendons in the leg that are too tight. Achilles tendon injuries are common in people who participate in the following sports. Running. Gymnastics. Dance. Football. Baseball. Softball. Basketball. Tennis. Volleyball. You are more likely to tear an Achilles tendon when you start moving suddenly. For instance, a sprinter might get one at the start of a race. The abrupt tensing of the muscle can be too much for the tendon to handle. Men older than age 30 are particularly prone to Achilles tendon injuries. Symptoms When the Achilles tendon ruptures a loud bang or popping sound may be heard. The person may feel that they have been hit or kicked in the back of the lower leg and often they will look over their shoulder to see who or what has hit them. This is quickly followed by the sudden onset of sharp pain in the tendon and a loss of strength and function. If a complete rupture has occurred it may not be possible to lift the heel off the ground or point the toes. Often the degree of pain experienced, or lack of it, can be inversely proportional to the extent of the injury, ie a partial rupture may in fact be more painful than a complete rupture. Diagnosis If an Achilles tendon rupture is suspected, it is important to consult a doctor straight away so that an accurate diagnosis can be made and appropriate treatment recommended. Until a doctor can be consulted it is important to let the foot hang down with the toes pointed to the ground. This prevents the ends of the ruptured tendon pulling any farther apart. The doctor will take a full medical history, including any previous Achilles tendon injuries and what activity was being undertaken at the time the present injury occurred. The doctor will also conduct a physical examination and will check for swelling, tenderness and range of movement in the lower leg and foot. A noticeable gap may be able to be felt in the tendon at the site of the rupture. This is most obvious just after the rupture has occurred and swelling will eventually make this gap difficult to feel. One test commonly used to confirm an Achilles tendon rupture is the Thomson test. For this test the patient lies face down on an examination table. The doctor then squeezes the calf muscles; an action that would normally cause the foot to point like a ballerina (plantar flexion). When a partial rupture has occurred the foot's ability to point may be decreased. When a complete rupture has occurred, the foot may not point at all. Ultrasound scanning of the Achilles tendon may also be recommended in order to assist with the diagnosis. Non Surgical Treatment Medical therapy for a patient with an Achilles tendon rupture consists of rest, pain control, serial casting, and rehabilitation to maximize function. Ongoing debate surrounds the issue of whether medical or surgical therapy is more appropriate for this injury. Conservative management of Achilles tendinosis and paratenonitis includes the following. Physical therapy. Eccentric exercises are the cornerstone of strengthening treatment, with most patients achieving 60-90% pain relief. Orthotic therapy in Achilles tendinosis consists of the use of heel lifts. Nonsteroidal anti-inflammatory drugs (NSAIDs). Tendinosis tends to be less responsive than paratenonitis to NSAIDs. Steroid injections. Although these provide short-term relief of painful symptoms, there is concern that they can weaken the tendon, leading to rupture. Vessel sclerosis. Platelet-rich plasma injections. Nitric oxide. Shock-wave therapy. Pain of the Achilles tendon commonly affects both competitive and recreational athletes, and the sedentary. The largest tendon in the body, the Achilles tendon, endures strain and risks rupture from running, jumping, and sudden acceleration or deceleration. Overuse, vascular diseases, neuropathy, and rheumatologic diseases may cause tendon degeneration. The hallmarks of Achilles tendon problems seem to be damaged, weak, inelastic tissue. Causes An Achilles tendon injury might be caused by several factors. Overuse. Stepping up your level of physical activity too quickly. Wearing high heels, which increases the stress on the tendon. Problems with the feet, an Achilles tendon injury can result from flat feet, also known as fallen arches or overpronation. In this condition, the impact of a step causes the arch of your foot to collapse, stretching the muscles and tendons. Muscles or tendons in the leg that are too tight. Achilles tendon injuries are common in people who participate in the following sports. Running. Gymnastics. Dance. Football. Baseball. Softball. Basketball. Tennis. Volleyball. You are more likely to tear an Achilles tendon when you start moving suddenly. For instance, a sprinter might get one at the start of a race. The abrupt tensing of the muscle can be too much for the tendon to handle. Men older than age 30 are particularly prone to Achilles tendon injuries. Symptoms When the Achilles tendon ruptures a loud bang or popping sound may be heard. The person may feel that they have been hit or kicked in the back of the lower leg and often they will look over their shoulder to see who or what has hit them. This is quickly followed by the sudden onset of sharp pain in the tendon and a loss of strength and function. If a complete rupture has occurred it may not be possible to lift the heel off the ground or point the toes. Often the degree of pain experienced, or lack of it, can be inversely proportional to the extent of the injury, ie a partial rupture may in fact be more painful than a complete rupture. Diagnosis If an Achilles tendon rupture is suspected, it is important to consult a doctor straight away so that an accurate diagnosis can be made and appropriate treatment recommended. Until a doctor can be consulted it is important to let the foot hang down with the toes pointed to the ground. This prevents the ends of the ruptured tendon pulling any farther apart. The doctor will take a full medical history, including any previous Achilles tendon injuries and what activity was being undertaken at the time the present injury occurred. The doctor will also conduct a physical examination and will check for swelling, tenderness and range of movement in the lower leg and foot. A noticeable gap may be able to be felt in the tendon at the site of the rupture. This is most obvious just after the rupture has occurred and swelling will eventually make this gap difficult to feel. One test commonly used to confirm an Achilles tendon rupture is the Thomson test. For this test the patient lies face down on an examination table. The doctor then squeezes the calf muscles; an action that would normally cause the foot to point like a ballerina (plantar flexion). When a partial rupture has occurred the foot's ability to point may be decreased. When a complete rupture has occurred, the foot may not point at all. Ultrasound scanning of the Achilles tendon may also be recommended in order to assist with the diagnosis. Non Surgical Treatment Medical therapy for a patient with an Achilles tendon rupture consists of rest, pain control, serial casting, and rehabilitation to maximize function. Ongoing debate surrounds the issue of whether medical or surgical therapy is more appropriate for this injury. Conservative management of Achilles tendinosis and paratenonitis includes the following. Physical therapy. Eccentric exercises are the cornerstone of strengthening treatment, with most patients achieving 60-90% pain relief. Orthotic therapy in Achilles tendinosis consists of the use of heel lifts. Nonsteroidal anti-inflammatory drugs (NSAIDs). Tendinosis tends to be less responsive than paratenonitis to NSAIDs. Steroid injections. Although these provide short-term relief of painful symptoms, there is concern that they can weaken the tendon, leading to rupture. Vessel sclerosis. Platelet-rich plasma injections. Nitric oxide. Shock-wave therapy. 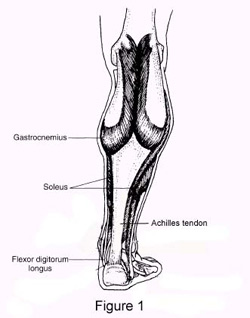 Surgical Treatment Surgery for Achilles tendon rupture requires an operation to open the skin and physically suture (sew) the ends of the tendon back together, has a lower incidence of re-rupture than nonsurgical treatment. Allows return to pre-injury activities sooner and at a higher level of functioning with less shrinkage of muscle. Risks are associated with surgery, anesthesia, infection, skin breakdown, scarring, bleeding, accidental nerve injury, higher cost, and blood clots in the leg are possible after surgery. Surgery has been the treatment of choice for the competitive athlete or those with a high level of physical activity, for those with a delay in treatment or diagnosis, and for those whose tendons have ruptured again. Surgical Treatment Surgery for Achilles tendon rupture requires an operation to open the skin and physically suture (sew) the ends of the tendon back together, has a lower incidence of re-rupture than nonsurgical treatment. Allows return to pre-injury activities sooner and at a higher level of functioning with less shrinkage of muscle. Risks are associated with surgery, anesthesia, infection, skin breakdown, scarring, bleeding, accidental nerve injury, higher cost, and blood clots in the leg are possible after surgery. Surgery has been the treatment of choice for the competitive athlete or those with a high level of physical activity, for those with a delay in treatment or diagnosis, and for those whose tendons have ruptured again.
Overview
 About two thirds of all Achilles tendon ruptures occur during sports. Total ruptures are most common in sports with stop-and-go movements, especially ball sports. The majority of patients suffered a ruptured Achilles tendon when stopping suddenly during a fast vigorous movement. Usually the Achilles tendon tears about 5 cm before it inserts into the heel bone. Particularly at risk for a tear are athletes who have already suffered from Achilles tendon problems for some time. About two thirds of all Achilles tendon ruptures occur during sports. Total ruptures are most common in sports with stop-and-go movements, especially ball sports. The majority of patients suffered a ruptured Achilles tendon when stopping suddenly during a fast vigorous movement. Usually the Achilles tendon tears about 5 cm before it inserts into the heel bone. Particularly at risk for a tear are athletes who have already suffered from Achilles tendon problems for some time.Causes The cause of Achilles tendon ruptures besides obviously direct trauma, is multifactorial. In many instances the rupture occurs about 2-6 cm before its attachment to the calcaneous (heel bone). In this area there is a weaker blood supply making it more susceptible to injury and rupture. Rigid soled shoes can also be the causative factor in combination with the structure of your foot being susceptible to injury. Symptoms If your Achilles tendon is ruptured you will experience severe pain in the back of your leg, swelling, stiffness, and difficulty to stand on tiptoe and push the leg when walking. A popping or snapping sound is heard when the injury occurs. You may also feel a gap or depression in the tendon, just above heel bone. Diagnosis The actual area of an Achilles tendon rupture cannot be seen on x-ray. Therefore, although x-rays are often done to rule out bony injuries in individuals with an Achilles tendon rupture these x-rays are usually normal. Diagnostic ultrasound of the tendon can be performed to assess the integrity of the tendon. Other diagnostic tests, such as MRI's, may also be required in difficult cases. Non Surgical Treatment The most widely used method of non-surgical treatment involves the use of serial casting with gradual progression from plantar flexion to neutral or using a solid removable boot with heel inserts to bring the ends of the tendon closer together. The advantage of a solid removable boot is that it allows the patient to begin early motion and is removable. Wide variability exists among surgeons in regards to the period of absolute immobilization, initiating range of motion exercises, and progression of weight bearing status.  Surgical Treatment Surgery is recommended to those who are young to middle-aged and active. The ruptured tendon is sewn together during surgery. This is an outpatient procedure. Afterward the leg is put into a splint cast or walking boot. Physical therapy will be recommended. In about 4 to 6 months, healing is nearly complete. However, it can take up to a year to return to sports fully. Prevention The best treatment of Achilles tendonitis is prevention. Stretching the Achilles tendon before exercise, even at the start of the day, will help to maintain ankle flexibility. Problems with foot mechanics can also lead to Achilles tendonitis. This can often be treated with devices inserted into the shoes such as heel cups, arch supports, and custom orthotics. |
